Tests
Gram Stain Test: What It Detects and How It Works
Infectious disease management relies heavily on the rapid differentiation of pathogens to initiate appropriate therapeutic interventions. Since its development by Hans Christian Gram in 1884, the classification method bearing his name has served as a primary diagnostic tool in microbiology laboratories globally: the Gram Stain Test.
Clinicians utilise the technique to categorise bacteria into Gram-positive or Gram-negative groups based on cell wall properties, directly influencing empiric antibiotic selection before culture data becomes available. For pathologists, knowing the biochemical principles, a procedural methodology, and the clinical significance of the test results is imperative to ensure accurate diagnostic workflows. Let us explore them in this article.
Why the Gram Stain Test
The Gram stain test is a basic assay in the pathology laboratory. It classifies bacteria based on the structural integrity and composition of their cell walls. By exploiting the differences in peptidoglycan thickness, the stain allows pathologists to differentiate between two major bacterial groups: Gram-positive and Gram-negative.
The differentiation provides immediate clinical value, as it assists treating physicians in narrowing down potential pathogens and selecting the most effective antibiotic regimen.
The test also gives insight into the severity of an infection. For instance, the presence of numerous bacteria alongside inflammatory cells indicates a robust infectious process. Conversely, a sample showing few bacteria might suggest colonisation rather than active infection, or a lower bacterial load.
Biological Basis: The Cell Wall Difference
The core mechanism of the Gram stain test centres on the interaction between the bacterial cell wall and specific dyes.
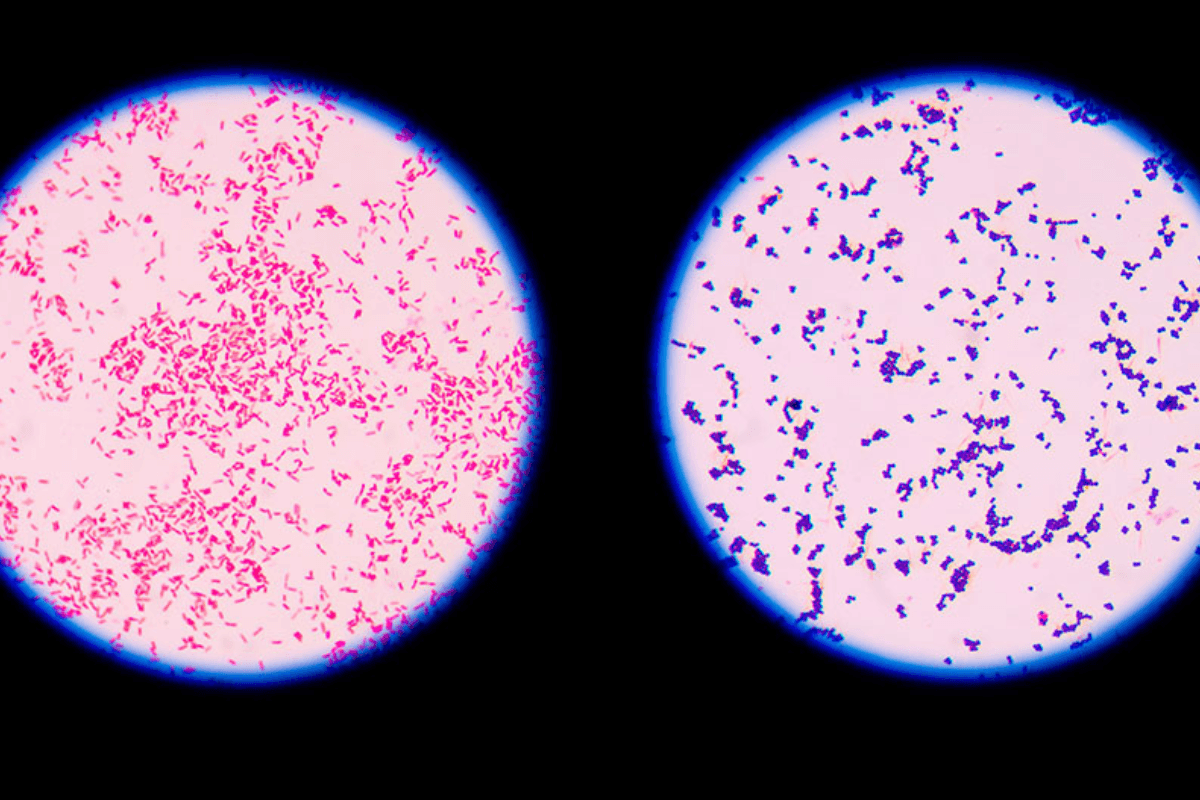
Gram-Positive Bacteria
These organisms possess a thick layer of peptidoglycan in their cell walls. During the staining process, the thick layer retains the initial crystal violet dye-iodine complex. Consequently, these bacteria appear purple or blue under microscopic examination. MRSA, streptococcal infections, and toxic shock syndrome are some of the common pathologies associated with the.
Gram-Negative Bacteria
These bacteria feature a much thinner peptidoglycan layer surrounded by an outer lipid membrane. The alcohol wash step disrupts the outer membrane and washes away the crystal violet. These cells then take up the counterstain (safranin), appearing pink or red. Pathogens in this category include Salmonella and organisms causing meningitis, gonorrhea, and pneumonia.
Detailed Procedure and Slide Preparation
To ensure a valid Gram stain report, adherence to strict procedural protocols is mandatory. The process begins with sample collection and extends to microscopic analysis.
1. Sample Collection
The efficacy of the test depends on the quality of the specimen. Common sources include:
- Sterile Fluids: Blood, cerebrospinal fluid, and joint fluid.
- Non-Sterile Sites: Sputum, throat swabs, and wounds.
- Excretions: Urine (clean-catch midstream is required).
For sputum samples, patients should avoid eating or drinking immediately prior to collection to minimise contamination. Wounds require sterile collection techniques to avoid commensal skin flora.
2. Staining Methodology
Once a thin smear is prepared and fixed on a slide, the four-step staining protocol is followed.
- Primary Stain: Crystal violet is applied, staining all bacteria purple.
- Mordant: Iodine is added to fix the dye within the cell wall structure.
- Decolourisation: An alcohol or acetone wash is used. This step differentiates the bacteria; Gram-positive cells retain the purple hue, while Gram-negative cells lose it.
- Counterstain: Safranin is applied to colour the now-colourless Gram-negative bacteria pink or red.
Gram Stain Interpretation and Reporting
Pathologists must analyse the slide for colour, shape, and arrangement. A complete Gram stain interpretation guides the correct diagnosis.
Summary of Gram Stain Results
| Observation | Appearance | Interpretation | Common Examples |
|---|---|---|---|
| Gram-Positive | Purple/Blue | Thick peptidoglycan wall | Staphylococci, Streptococci, Listeria |
| Gram-Negative | Pink/Red | Thin wall, outer membrane | E. coli, Pseudomonas, Neisseria |
| Yeast/Fungi | Purple (Variable) | Large, budding cells | Candida species |
| Pus Cells | Pink Nuclei | Inflammatory response | Neutrophils / Leukocytes |
| Epithelial Cells | Pink | Skin/mucosa contamination | Squamous cells |
Bacterial Morphology and Arrangement
The Gram staining observation process identifies the shape of the bacteria:
- Cocci: Round or spherical.
- Bacilli: Rod-shaped.
The arrangement provides further clues. For example, a staph-aureus Gram stain reveals Gram-positive cocci in clusters (grape-like), whereas Streptococcus species appear in chains or pairs.
Analysing the Gram Stain Report
- Gram Stain Test Positive: This indicates the presence of bacteria. The report will specify the type (e.g., "Gram-positive cocci in pairs").
- No Organisms Seen: A "normal" result where no pathogenic bacteria are visible. This suggests a non-bacterial aetiology or a bacterial load below the detection threshold.
- Pus Cells in Gram Stain: The presence of polymorphonuclear leukocytes (pus cells) signifies an active immune response and inflammation at the infection site.
- Occasional Gram-Negative Bacilli Seen: This phrasing indicates a lower quantity of rod-shaped, pink-staining bacteria, which might be significant depending on the sample source (e.g., sterile spinal fluid vs. non-sterile sputum).
- Gram Positive Cocci in Urine: Finding these organisms in a urine sample can indicate a urinary tract infection caused by Enterococcus or Staphylococcus species.
Non-Bacterial Findings
While primarily for bacteria, the test has broader utility. A fungal Gram stain can detect yeast or mould. Yeast cells often appear as large, purple, budding structures, distinct from bacteria due to their size and morphology.
Factors Affecting Accuracy and Limitations
- Gram stain has limitations and works mainly as a screening tool, not a definitive identification method.
- Antibiotic interference can cause false negatives because starting antibiotics before sample collection may degrade bacterial cell walls or reduce the bacterial load.
- Fastidious organisms may not stain reliably.
- Gram stain is ineffective for TB (tuberculosis) because Mycobacterium tuberculosis has a waxy cell wall that resists normal dyes; acid-fast staining is required instead.
- Sputum contaminated with saliva may show mixed flora, making it harder to identify the true pathogen.
- Mixed infections containing both Gram-negative and Gram-positive bacteria require careful differentiation.
Closure
A Gram stain test serves as the initial piece of the diagnosis. However, it does not identify the specific bacterial species or its antibiotic susceptibility profile. Culture and sensitivity testing must follow the Gram stain to confirm the diagnosis.
Healthcare professionals must interpret Gram stain results in conjunction with patient symptoms and medical history. By understanding the nuances of the test, pathology teams can provide the essential data required for effective patient management.
Also check - Bacitracin Sensitivity Test: Uses and Interpretation Guide
Get Started at ₹1!
Try Flabs for a full month for just ₹1.
Follow us on