Flabs
Blood Grouping and Cross-Matching: Procedure and Importance
In transfusion medicine, precision is the only currency that matters. You know the stakes. One clerical error or a missed antibody can turn a life-saving procedure into a catastrophic event. For pathologists and laboratory professionals, the routine nature of these tests never diminishes their gravity. We deal with biological variability daily, yet the expectation remains absolute accuracy.
Let’s get into the nuances of blood grouping and cross-matching, examining the protocols that keep our patients safe and our laboratories compliant.
Blood Grouping and Cross-Matching: The Clinical Imperative
Why do we run these tests with such rigour? It is not just about identifying Type A or Type B. It is about biological compatibility in its strictest sense. The primary goal is to prevent immediate and delayed hemolytic transfusion reactions.
We know that accurate blood grouping and cross-matching before transfusion prevents the immune system from launching an attack on donor cells, which can lead to shock, renal failure, or worse.
Beyond emergencies, the indications of blood grouping and cross-matching extend to prenatal care to assess Rh incompatibility, organ transplantation, and preoperative assessments for major surgeries where blood loss is anticipated. Every sample represents a patient relying on our technical competence.
Distinguishing the Two
Professionals must articulate the difference between blood grouping and cross-matching clearly to clinical staff who might view them as a single checkbox. These are distinct processes.
Blood grouping determines the specific antigens present on the red blood cell surface. It defines the donor and recipient's ABO and Rh status. Think of it as checking the ID card of the blood.
Cross-matching is the trial run. It mimics the transfusion in a test tube or microplate to see if the recipient’s serum reacts with the donor’s red cells. It catches what grouping might miss. Specifically, irregular antibodies outside the ABO system.
The Procedure
Standardisation is our safety net. A robust blood grouping and cross-matching procedure begins long before the sample hits the analyser. It starts at the bedside.
Pre-Analytical Considerations
Errors frequently occur during the blood grouping and cross-matching blood collection phase.
- Tube mislabeling is a critical error that cannot be corrected by any advanced technology.
- Positive patient identification is mandatory.
- EDTA-anticoagulated samples are required to prevent in vitro complement activation.
- Failure to use EDTA may result in false-positive test results.
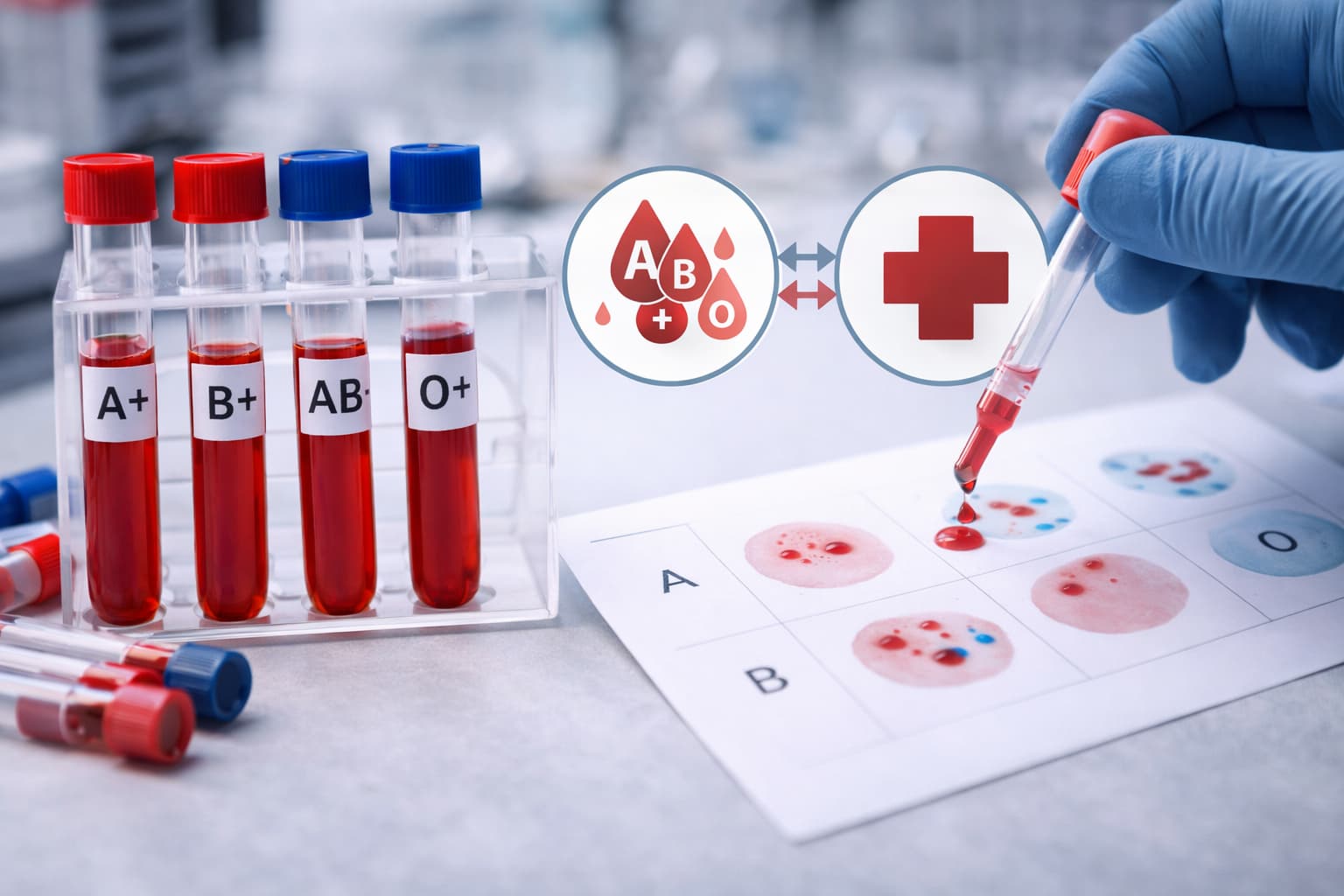
Step 1: ABO and Rh Typing
The ABO blood grouping and cross-matching protocol is the first line of defence.
- Forward Grouping (Cell Grouping): We mix patient RBCs with Anti-A and Anti-B reagents. Agglutination signals the presence of the corresponding antigen.
- Reverse Grouping (Serum Grouping): We mix patient serum with known pooled A and B cells. This confirms the forward grouping results. Discrepancies here halt the process immediately until they are resolved.
- Rh Typing: We test for the D antigen. Weak D testing may be required for donors or prenatal patients to ensure we don't misclassify someone as Rh negative.
Step 2: Antibody Screening
Before moving to the cross-match, we screen the recipient's serum for unexpected alloantibodies using a panel of O cells with known antigen profiles.
If positive, identification is necessary to find antigen-negative donor units.
Step 3: The Cross-Match
- Major Cross-Match: Recipient serum against Donor RBCs. It detects antibodies in the patient that could destroy the transfused blood.
- Minor Cross-Match: Donor serum against Recipient RBCs. This has become less common in modern practice due to the use of packed red cells with minimal plasma volume.
Methodologies in the Modern Lab
The methods of blood grouping and cross-matching have evolved from simple glass slides to high-throughput automation.
1. Tube Method
It has been the gold standard for decades. While it is reliable and flexible, it is labour-intensive. It relies heavily on the technologist’s skill in reading agglutination strength.
2. Column Agglutination Technology (CAT)
Often called the "Gel Card" method. It standardises the reading. RBCs filter through a gel matrix. Agglutinated cells get trapped at the top, while free cells pass to the bottom. It gives out a stable endpoint that another tech can review later.
3. Solid Phase Red Cell Adherence (SPRCA)
Used primarily in automated systems. Microplates are coated with reagents. Positive reactions show a monolayer of cells adhering to the well surface.
| Feature | Tube Method | Gel Card (CAT) | Solid Phase (SPRCA) |
|---|---|---|---|
| Sensitivity | Moderate | High | High |
| Objectivity | Subjective (Reader dependent) | Objective | Objective (Automated reading) |
| Sample Volume | Larger volume required | Microsamples sufficient | Microsamples sufficient |
| Archive | Difficult to store results physically | Cards can be photographed/stored | Digital storage |
| Throughput | Low | Medium to High | Very High |
| Cost | Low reagent cost | Moderate | High initial investment |
Automation and Efficiency
Many pathology labs in India and globally are transitioning to full automation to handle increasing volumes. A modern blood grouping and cross-matching machine integrates sampling, incubation, centrifugation, and reading.
These systems interface directly with Laboratory Information Systems (LISs) like Flabs. This integration reduces transcription errors significantly. Automation also improves turnaround time.
While a manual stat cross-match might take 45 minutes to an hour, depending on antibody status, automated systems can batch samples efficiently. It also up technicians to focus on complex problem-solving like antibody identification.
However, automation does not replace expertise. A machine might flag a result as "indeterminate." A skilled pathologist must then step in. We interpret the mixed-field reactions. We troubleshoot the cold agglutinins. We decide when to override a flag or request a fresh sample.
Equipment and Infrastructure
Investing in the right pathology lab equipment is an investment in patient safety. Beyond the analysers, we need:
- Calibrated centrifuges (for the tube method).
- Dedicated reagent refrigerators with continuous temperature monitoring.
- Cell washers to remove plasma proteins.
- Microscopes for confirming weak reactions.
Maintenance logs are not just paperwork. They are proof that our tools are functioning within defined parameters.
Challenges in the Lab
Every day brings a new puzzle. We encounter samples with autoantibodies that react with everything. We see patients who have received multiple transfusions and developed a cocktail of antibodies.
In these cases, "stat" requests become stressful. Communicating realistic timelines to clinicians is part of the job. We cannot rush biology. If an antibody needs identification, it will take time. Rushing leads to shortcuts. Shortcuts lead to errors.
Another challenge is the "massive transfusion" scenario. When a patient bleeds out, we may not have time for a full cross-match. We switch to emergency release protocols (O Negative uncross-matched). Documentation becomes vital here. We must record that the risk was acknowledged by the treating physician.
The Future
We are moving toward molecular methods. Genotyping allows us to predict phenotypes based on DNA. This is particularly useful for multiply transfused patients where serological phenotyping is impossible due to the presence of donor cells.
While serology remains the workhorse, molecular testing will likely become more accessible. It offers precision that agglutination simply cannot match.
Final Thoughts
The science of blood grouping and cross-matching is a blend of rigid protocol and expert judgment. It sits at the intersection of immunology and genetics. For those of us in the lab, it is never just a test. It is a commitment to the patient on the other side of that sample tube. We ensure that the gift of blood remains a gift of life, not a source of harm.
Technology will advance. Methods will shift. But the core principle remains: absolute certainty before the infusion begins.
Also check - Blood Group Test Procedure & Importance Explained
Get Started at ₹1!
Try Flabs for a full month for just ₹1.
Follow us on