Tests
Mantoux Test: Procedure, Purpose & Interpretation
Tuberculosis (TB) latency presents one of the trickier puzzles in infectious disease pathology. While newer assays exist, the Mantoux test is a primary screening tool for identifying Mycobacterium tuberculosis infection. It relies on a hypersensitivity reaction that, while simple in principle, requires precision in execution and interpretation.
We know you don't need a basic biology lesson. Instead, we will focus on the technical nuances of the Tuberculin Skin Test (TST), managing false variances, and the specific clinical thresholds determining positivity.
What Is the Mantoux Test?
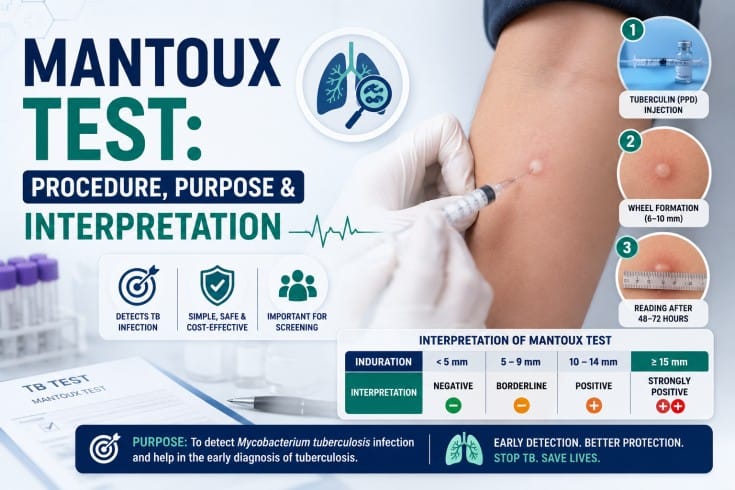
The Mantoux test, also known as the Tuberculin Skin Test (TST), is a screening test used to detect tuberculosis (TB) infection. It involves injecting a small amount of purified protein derivative (PPD) under the skin and measuring the size of the skin reaction after 48–72 hours to determine whether a person has been exposed to Mycobacterium tuberculosis.
The Mantoux test is commonly used to:
- Screen for latent tuberculosis (TB) infection
- Support TB diagnosis along with clinical evaluation and other tests
- Identify individuals at increased risk of developing active TB
Why We Still Rely on TST
Despite the rise of interferon-gamma release assays (IGRAs), the skin test holds its ground. Cost-effectiveness drives its widespread use in resource-limited settings and large-scale public health screenings.
The Mantoux test is used for the diagnosis of latent TB infection (LTBI) primarily, acting as a gatekeeper before clinicians order chest radiography or initiate prophylactic therapy.
You also encounter it during contact tracing. When an active pulmonary TB case surfaces, identifying exposed individuals quickly becomes priority number one. The TST is a functional, immediate way to assess immune sensitisation in these cohorts.
The Administration Protocol
Standardisation prevents data skew. Administering the Mantoux tuberculin skin test involves strict adherence to the intradermal injection technique. Deviating from the protocol introduces variables that make your final read unreliable.
Preparation: Use a purified protein derivative (PPD) solution. Standard dosing involves 5 tuberculin units (TU) of PPD-S in 0.1 mL of solution.
Site Selection: Locate the volar surface of the forearm. Avoid areas with veins, rashes, or heavy hair growth.
Injection: Insert the needle bevel-up at a 5 to 15-degree angle. You must place the PPD just below the skin surface.
Verification: A pale elevation of the skin (a wheal) measuring 6 mm to 10 mm in diameter should appear immediately. If you don't see a wheal, or if significant bleeding occurs, the injection went too deep. You will need to repeat the test at a different site.
The Reading Window
Timing dictates accuracy. The Mantoux test reading time falls strictly between 48 and 72 hours post-injection. Examining the arm before 48 hours leads to false negatives because the delayed-type hypersensitivity reaction hasn't peaked. Waiting past 72 hours allows the reaction to fade, degrading the signal.
Instruct patients to return within this window. If they miss it, you have no choice but to restart the process. Safety dictates that you cannot simply guess based on a fading mark.
Distinguishing Induration from Erythema
Here lies the most common error in Mantoux test interpretation. When you measure induration (the palpable, raised hardening), not erythema (the redness). Redness essentially tells you nothing about the immune burden.
- Inspect the arm under good light.
- Palpate the area with your fingertips to find the margins of the induration.
- Mark the edges with a ballpoint pen across the forearm axis.
- Measure the distance between the pen marks using a millimetre ruler.
Record the result in millimetres, even if it measures 0 mm. "Negative" is not a measurement; "0 mm" is data.
Defining Positivity: The Cutoff Points
What constitutes a positive Mantoux test result depends entirely on the patient's risk profile. We do not use a single "positive" number. Instead, we apply a stratified approach to sensitivity.
Patients might ask about the Mantoux test normal range, assuming a universal baseline exists. You know it doesn't. We evaluate results against specific thresholds, e.g., 5 mm, 10 mm, and 15 mm.
5 mm or More
We consider an induration of 5 mm or larger positive for the highest risk groups. Their immune systems may not mount a massive reaction, so we lower the bar to catch the infection.
- HIV-infected persons.
- Recent contacts of persons with infectious TB disease.
- Persons with fibrotic changes on chest radiographs consistent with prior TB.
- Patients with organ transplants.
- Individuals on immunosuppressive therapy (e.g., TNF-alpha antagonists).
10 mm or More
For those with elevated risk but intact immunity, we raise the threshold.
- Recent immigrants from high-prevalence countries.
- Injection drug users.
- Residents and employees of high-risk congregate settings (prisons, nursing homes, hospitals).
- Mycobacteriology laboratory personnel.
- Children under 4 years of age.
- Children are exposed to adults in high-risk categories.
15 mm or More
In persons with no known risk factors for TB, we demand a strong reaction to classify it as positive.
- General population with no exposure history.
- Note: Targeted skin testing programs should only be conducted among high-risk groups. Testing low-risk individuals diverts resources and increases the risk of false positives.
| Induration Size | Risk Group Classification | Clinical Implication |
|---|---|---|
| ≥ 5 mm | HIV-positive individuals, recent TB contacts, organ transplant recipients, immunosuppressed patients | Considered positive due to high susceptibility or a reduced ability to mount a strong immune response. |
| ≥ 10 mm | Recent immigrants (within the last 5 years), laboratory personnel, children under 4 years, injection drug users, residents of congregate settings | Considered positive due to increased environmental or behavioural exposure to tuberculosis. |
| ≥ 15 mm | Individuals with no known TB risk factors | Considered positive only because the reaction is significant. Routine testing of this group is generally not recommended. |
Addressing False Positives and Negatives
The TST is not infallible. Several factors complicate the picture.
The BCG Factor
Many patients from outside the US received the Bacillus Calmette-Guérin (BCG) vaccine. This creates cross-reactivity. A history of BCG vaccination can cause a false-positive reaction. However, current guidelines suggest you generally ignore BCG history when interpreting TST results. If the induration meets the diagnostic cutoff, treat it as a latent infection until proven otherwise.
The Booster Phenomenon
Over time, the ability to react to tuberculin wanes. If you test an older adult whose infection occurred decades ago, the initial skin test might be negative. The test itself, however, stimulates the immune system. If you retest them a week later, they might show a positive reaction. We call this the booster effect. It mimics a recent conversion but actually represents restored immune memory. For healthcare worker baseline testing, use a two-step testing protocol to rule this out.
False Negatives
A negative result does not always guarantee freedom from infection. Viral infections (like measles or varicella), live virus vaccinations, or overwhelming TB disease (anergy) can suppress the immune response.
TST vs. IGRA
Patients and even some junior staff might refer to a Mantoux blood test. This phrasing conflates two different modalities. The Mantoux is strictly a skin test. They are likely looking for the Interferon-Gamma Release Assay (IGRA), such as QuantiFERON-TB Gold.
Unlike the TST, IGRAs require a single blood draw and do not cross-react with the BCG vaccine. They measure the T-cell release of interferon-gamma in response to specific M. tuberculosis antigens.
While IGRAs offer higher specificity in BCG-vaccinated populations, the TST generally costs less and requires no specialised laboratory equipment beyond a ruler and a trained eye. You might use an IGRA to confirm a positive TST in a low-risk individual or a BCG-vaccinated patient to rule out a false positive.
Procedural Nuance Matters
Diagnostic accuracy begins with your technique. A sloppy injection or a guessed measurement compromises the entire workflow.
When you ensure precise administration and strict adherence to reading windows, you transform a century-old tool into a reliable data point. The Mantoux test procedure is a fundamental skill in pathology and infectious disease management.
Suggested article IGRA Test: Tuberculosis Detection Explained
Get Started at ₹1!
Try Flabs for a full month for just ₹1.
Follow us on