Flabs
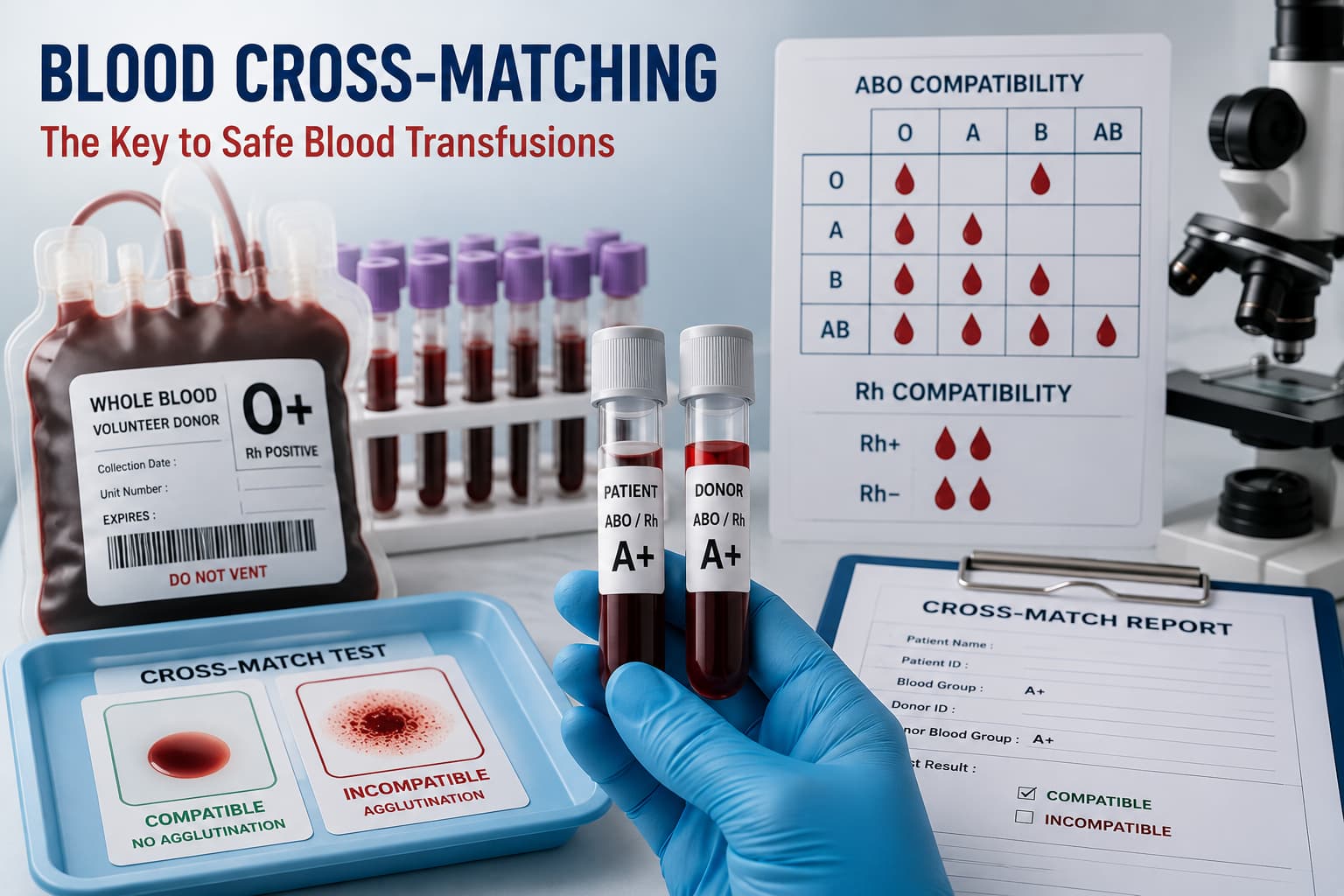
Blood Cross-Matching: Importance in Safe Blood Transfusions
Every year, thousands of patients receive blood transfusions. Most go smoothly. Some don't. And the ones that don't can kill within minutes. Acute haemolytic transfusion reactions driven by ABO or other blood group incompatibilities are one of the leading causes of mortality. The test designed to catch incompatibilities before they reach the patient is blood cross-matching.
If you work in a blood bank or pathology lab, you're already running the test dozens of times a week. But it's worth revisiting what the procedure actually does, where it can fail, and how lab systems can reduce the risk of error at scale.
What Is Blood Cross-Matching?
Blood cross-matching is a pre-transfusion compatibility test. It is performed in a blood bank to confirm that donor blood and recipient blood will not react adversely when mixed. It's the last safety checkpoint before releasing blood for transfusion that directly saves lives.
Even when blood grouping and cross-matching results appear aligned on paper, alloantibodies from prior pregnancies, previous transfusions, or underlying conditions can cause a reaction that ABO/Rh typing alone won't detect. Blood cross-matching picks up those antibodies in a live mixing environment.
Blood typing tells you which blood group you have.
Blood cross-matching tells you whether this specific donor unit is safe for this specific patient at this time.
Major and Minor Blood Cross-Matching
There are two components to a complete cross-match. You need to know both, because they test for different failure modes.
| Type | What You Mix | What It Detects |
|---|---|---|
| Major Cross-Matching of Blood | Donor RBCs + Recipient Serum/Plasma | Recipient antibodies against donor red cell antigens |
| Minor cross-matching | Recipient RBCs + Donor Serum/Plasma | Donor antibodies against recipient red cell antigens |
| Auto Control | Patient RBCs + Patient Serum | Autoantibodies or coating of the patient’s own RBCs |
In most blood banks today, major cross-matching of blood is considered imperative. Minor cross-matching has become less routine for packed RBC transfusions since donor plasma is minimal. But for whole blood or granulocyte products, it still carries weight.
The Blood Cross-Matching Procedure: Step by Step
The blood cross-matching procedure follows a defined sequence. Deviations at any step can produce false negatives with serious consequences.
1. Sample and Labelling: Collect the recipient's EDTA and clotted blood samples. Label at the bedside, not later at the bench. A labelling error here is the single most common cause of transfusion fatality.
2. ABO/Rh: Recheck ABO and Rh grouping on the current sample before proceeding to the cross-match.
3. Antibody Screening: Screen recipient serum for clinically significant alloantibodies using a panel of reagent RBCs.
4. Prepare cell suspensions: Prepare a 2–5% saline suspension of donor RBCs from the segment attached to the blood bag.
5. Immediate spin phase: Mix donor RBCs with recipient serum, centrifuge, and read for agglutination or haemolysis.
6. 37°C incubation: Incubate tubes at 37°C for 30–60 minutes to detect clinically significant warm-reactive antibodies.
7. Antiglobulin (AHG) phase: Wash cells, add anti-human globulin (Coombs reagent), centrifuge, and read. Add check cells (IgG-coated RBCs) to validate negative results.
8. Interpretation and Release: Document, interpret, and authorise blood unit release only after all phases are complete.
Note: The IAT (indirect antiglobulin test) phase is the most sensitive step. Never skip cell validation on negatives. A false-negative AHG result without check cells indicates an undetected test failure.
The Tube Method
The blood cross-matching tube method is the backbone of manual cross-matching in most labs. It's straightforward, uses a basic centrifuge, and gives you visual agglutination readings that experienced staff can interpret with high confidence.
In the tube method, you work through three phases in labelled glass or plastic tubes, viz., immediate spin, 37°C, and AHG.
Each phase targets a different antibody class based on thermal amplitude and Ig type. IgM antibodies (ABO, Lewis cold reactive) react in the immediate spin. IgG antibodies (Kell, Duffy, Kidd, Rh) need the AHG phase to become visible.
Gel card and solid-phase methods have been adopted by many labs for routine use. But in situations requiring urgent cross-matching or when discrepant results occur, the tube method is the confirmatory test.
Blood Cross-Matching Times
| Scenario | Method Used | Expected TAT |
|---|---|---|
| Elective surgery / planned transfusion | Full serological cross-match | 45–90 minutes |
| Urgent transfusion (non-emergency) | Abbreviated / immediate spin + electronic cross-match | 15–30 minutes |
| Emergency / massive haemorrhage | Emergency O-negative release (uncross-matched blood) | Immediate (< 5 min) |
| Electronic cross-match | Computer-based compatibility check (requires 2 prior blood group records) | Minutes |
| Neonatal cross-matching | Mother + infant sample required | 45–90 minutes |
Blood cross-matching time directly impacts patient care in trauma bays, surgical suites, and ICUs. Your blood bank's TAT for cross-match blood test completion needs to be tracked in real time. Any bottleneck has a clinical cost.
Direct Cross-Matching of Blood
Direct cross-matching of blood, where you physically mix donor and recipient samples and observe for agglutination or hemolysis, is the classic serological approach. It contrasts with the electronic (computer) cross-match, which relies on a database match of two concordant historical ABO/Rh typings without a physical serological step.
Direct cross-matching of blood is indicated in the following cases.
The patient has no prior typing history in your LIS.
Antibody screen is positive or clinically significant antibodies were previously detected.’
There are discrepancies in ABO typing.
You're transfusing neonates or patients with autoimmune conditions.
Local policy mandates serological confirmation regardless of electronic eligibility.
Never default to electronic cross-match for new patients or those with complex antibody histories. Direct serological testing protects where the electronic system, by design, cannot.
Equipment in the Blood Bank
Running a reliable cross-match at volume demands properly maintained pathology lab equipment. Your centrifuge calibration, incubator temperature logs, refrigerator monitoring for reagents, and coagulometer performance all feed into transfusion safety indirectly but meaningfully.
A coagulometer, for example, plays a role in parallel coagulation workups for patients receiving massive transfusions, where FFP and platelet needs are assessed alongside packed red cell compatibility. Keeping QC logs current on all equipment is a regulatory requirement and a patient safety measure.
Common Errors
| Error Type | Where It Occurs | Prevention |
|---|---|---|
| Wrong blood in tube (WBIT) | Phlebotomy / sample collection | Bedside labelling protocol, barcode scanning |
| Skipped check cells | AHG phase of tube method | SOP enforcement, automated LIS checks |
| Missed alloantibody | Antibody screen | Extended antigen typing for repeat transfusion patients |
| Transcription error in blood unit ID | Blood bank issue | Barcode verification at every handoff |
| Electronic cross-match on ineligible patient | LIS / blood bank staff | Rule-based LIS eligibility checks before approval |
Final Takeaways
Blood cross-matching is not a formality. It's a live biological test with direct patient safety implications where every step matters.
- Always run the major cross-matching of blood. It protects the patient from their own antibodies reacting with donor cells.
- Use the full AHG phase for patients with a positive antibody screen or complex history.
- Track your blood cross-matching time by request and act on TAT breaches immediately.
- Reserve electronic cross-match for eligible patients only.
- Keep your equipment QC logs current.
- Invest in an LIS that flags problems before they reach the patient.
FLABS LIS for Blood Banks & Pathology Labs
Cross-matching errors are not just technical. They’re clinical risks. The AI-Powered FLABS LIS helps you eliminate them at scale.
Automate compatibility checks, enforce cross-match eligibility rules, and flag critical exceptions in real time. From sample accessioning to final blood unit release, FLABS ensures traceability, faster TAT, and NABL-ready compliance without manual gaps.
Reduce transfusion risk. Improve cross-match TAT. Strengthen lab control.
Start Your 5-day Free Trial Today.