Flabs
Metaplasia vs Dysplasia: Key Differences Explained
Pathologists review cellular change every day. Some changes indicate adaptation, while others signal progression toward malignancy. Two terms appear frequently in histopathology reports: metaplasia and dysplasia.
Each represents a distinct biological process with different implications for diagnosis, surveillance, and clinical decisions.
Confusion between these processes still appears in training environments and clinical discussions. Clear differentiation improves medical reporting, communication, and patient management.
Metaplasia vs Dysplasia: At a Glance
| Feature | Metaplasia | Dysplasia |
|---|---|---|
| Definition | Reversible substitution of one mature differentiated cell type by another mature cell type better suited to tolerate stress. | Disordered cellular growth characterised by abnormal cell morphology, size, shape, and organisation within a tissue. |
| Nature of Change | Adaptive and protective response to chronic irritation or environmental stress. | Premalignant transformation indicating abnormal proliferation and maturation of cells. |
| Cell Type | One fully differentiated cell type is replaced by another differentiated cell type. | Same cell lineage persists but exhibits abnormal structural and functional characteristics. |
| Cellular Morphology | Cells appear normal for the new cell type; structural organisation is maintained. | Cells display pleomorphism, hyperchromatic nuclei, and abnormal architecture. |
| Underlying Mechanism | Stem cell reprogramming leads to differentiation into a different cell lineage better suited for the altered environment. | Genetic mutations and abnormal regulation of cell proliferation and differentiation. |
| Cellular Organisation | Tissue architecture is orderly and organised. | Loss of normal tissue architecture and cellular polarity. |
| Nuclear Changes | Nuclei remain normal in size, shape, and chromatin pattern. | Nuclear abnormalities such as hyperchromatism, enlarged nuclei, irregular nuclear membrane, increased nuclear-cytoplasmic ratio, and atypia. |
| Cell Proliferation | Normal rate of proliferation for the substituted cell type. | Increased and uncontrolled proliferation of abnormal cells. |
| Reversibility | Usually reversible when the underlying stimulus or irritant is removed. | Mild dysplasia may regress; moderate to severe dysplasia frequently progresses and may become irreversible. |
| Pathological Significance | Generally considered a benign adaptive change. | Considered a premalignant lesion with potential to progress to carcinoma in situ and invasive cancer. |
| Risk of Malignancy | Not inherently malignant but can predispose tissue to dysplasia if the stimulus persists. | High risk of malignant transformation if untreated. |
| Tissue Layers Affected | Entire epithelium replaced by another cell type without atypia. | Abnormal cells may involve the basal layers initially and extend through the full epithelial thickness in severe cases. |
| Effect on Tissue Function | May reduce original function but provides greater resistance to injury (e.g., loss of mucociliary clearance in the respiratory tract). | Function becomes impaired due to abnormal differentiation and disordered tissue structure. |
| Grading | Not graded because cells remain structurally normal. | Graded as mild, moderate, or severe based on the degree of cellular atypia and epithelial involvement. |
| Histological Appearance | Replacement epithelium resembles another normal tissue type. | Marked cellular atypia, mitotic figures, and disturbed maturation patterns. |
| Clinical Detection | Detected through histopathological examination or endoscopic biopsy. | Identified through cytology or histopathology (e.g., Pap smear for cervical dysplasia). |
| Common Causes | Chronic irritation, inflammation, smoking, vitamin deficiencies, hormonal influences. | Persistent carcinogenic stimuli such as viral infections, chronic inflammation, or chemical carcinogens. |
| Examples | Squamous metaplasia in bronchi of smokers; Barrett’s oesophagus (columnar metaplasia). | Cervical intraepithelial neoplasia (CIN), bronchial epithelial dysplasia in smokers. |
| Progression | Chronic metaplasia → may progress to dysplasia if irritant persists. | Dysplasia → carcinoma in situ → invasive carcinoma. |
| Clinical Management | Removal of the underlying stimulus and periodic monitoring. | Requires careful surveillance, biopsy evaluation, and sometimes surgical intervention. |
Metaplasia and Dysplasia
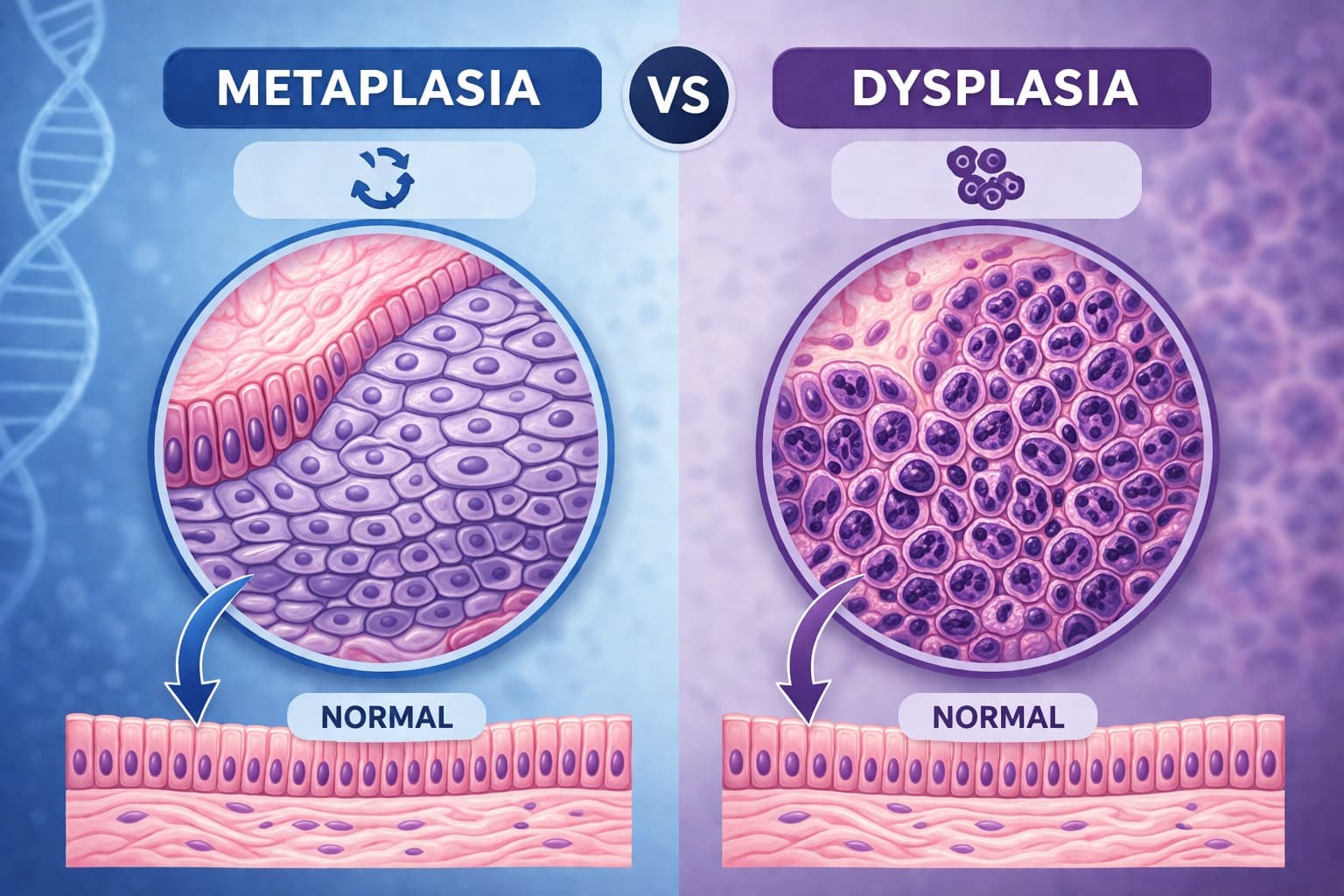
In diagnostic histopathology, metaplasia vs dysplasia describes two different forms of epithelial change. Both involve altered cellular architecture, yet biological intent and malignant potential differ.
Metaplasia represents an adaptive response. Dysplasia represents disordered growth with premalignant potential. Accurate interpretation during microscopic examination ensures precise pathology reporting.
When examining metaplasia vs dysplasia, there are three core elements.
- Cellular origin and differentiation.
- Architectural organisation.
- Potential progression toward carcinoma.
A pathologist reviewing metaplasia vs dysplasia evaluates these factors alongside clinical history, anatomical site, and exposure to chronic irritation.
Metaplasia Meaning in Pathology
The term metaplasia meaning refers to the replacement of one differentiated cell type by another mature cell type better suited to environmental stress.
Such a change occurs through stem cell reprogramming rather than direct conversion of mature cells. Environmental stimuli drive the shift. Chronic irritation, inflammation, hormonal changes, or chemical exposure act as triggers.
Classic examples include:
- Squamous metaplasia in bronchial epithelium among smokers.
- Intestinal metaplasia in gastric mucosa associated with chronic gastritis.
- Columnar metaplasia in the distal oesophagus during Barrett oesophagus.
During microscopic examination, metaplastic epithelium displays organised maturation and preserved polarity.
From a diagnostic standpoint, metaplasia indicates tissue adaptation. Removal of the irritant may allow tissue to revert or stabilise.
However, persistent injury may create conditions where dysplasia develops later.
Dysplasia Meaning in Histopathology
Dysplasia meaning describes disordered epithelial growth with cytologic atypia and architectural distortion.
Unlike adaptive metaplasia, dysplasia reflects abnormal proliferation. Genetic alterations accumulate within epithelial cells. Progressive degrees of atypia appear as lesions advance.
Microscopic characteristics include:
- Nuclear pleomorphism
- Hyperchromasia
- Increased nuclear-cytoplasmic ratio
- Loss of cellular polarity
- Increased mitotic figures
- Abnormal stratification
Dysplasia exists along a severity spectrum: Mild dysplasia, Moderate dysplasia, Severe dysplasia, Carcinoma in situ.
During evaluation of metaplasia vs dysplasia, dysplasia carries greater clinical concern because malignant transformation becomes possible.
Cellular Behaviour in Metaplasia and Dysplasia
A pathologist evaluating metaplasia vs dysplasia studies cellular behaviour rather than cell appearance alone.
Metaplasia shows organised replacement with preserved architecture. Dysplasia shows uncontrolled proliferation with architectural disruption.
Metaplasia: adaptive reprogramming of progenitor cells
Dysplasia: genetic instability with abnormal growth regulation
Chronic irritation may initiate metaplasia first. Continued exposure may later produce dysplasia within the altered epithelium. Such sequences appear in Barrett’s oesophagus and cervical transformation zones.
Microscopic Clues Pathologists Evaluate
While reviewing biopsy slides, several morphological clues assist in the evaluation of metaplasia vs dysplasia.
Look for patterns involving epithelial maturation, nuclear characteristics, and structural organisation.
- Degree of epithelial stratification.
- Nuclear size variation.
- Presence of mitotic activity above basal layers.
- Surface maturation patterns.
- Basal membrane integrity.
- Distribution of atypical cells.
A biopsy displaying organised differentiation favours metaplasia. Diffuse atypia with architectural disruption supports dysplasia.
Diagnostic interpretation of metaplasia vs dysplasia becomes stronger when morphological evidence aligns with clinical findings.
Relevance for Digital Pathology and Labs
Modern diagnostic practice integrates digital pathology, data management systems, and remote consultation. Growing networks of pathology labs in India manage increasing biopsy volumes across gastroenterology, gynaecology, and oncology.
Within such environments, standardised terminology for metaplasia vs dysplasia supports:
- Consistent reporting across laboratories.
- Smoother multidisciplinary communication.
- Reliable pathology databases for research.
Digital slide review platforms also allow subspecialty consultation when dysplasia grading becomes challenging.
Reliable documentation of metaplasia and dysplasia strengthens quality benchmarks in large laboratory networks.
Why Clear Distinction Matters
Misinterpretation between adaptive and premalignant changes may affect clinical decisions. For that reason, metaplasia vs dysplasia carries direct clinical impact.
- Dysplasia grading determines surveillance intervals.
- High-grade dysplasia may trigger surgical or endoscopic treatment.
- Metaplasia alone usually leads to monitoring rather than intervention.
Accurate microscopic evaluation protects patients from both overtreatment and delayed diagnosis.
During slide review, careful comparison of cytology and architecture clarifies metaplasia vs dysplasia even in borderline lesions.
Final Takeaway
For both pathologists and clinicians, clear differentiation between adaptive epithelial change and premalignant transformation shapes clinical management.
Metaplasia represents cellular adaptation to environmental stress. Dysplasia represents disordered growth with malignant potential.
When reviewing metaplasia vs dysplasia, focus on epithelial maturation, nuclear features, tissue architecture, and clinical context. Consistent terminology in pathology reports strengthens communication across multidisciplinary teams and large diagnostic networks.
Accurate interpretation of metaplasia vs dysplasia supports early detection of cancer risk while preventing unnecessary alarm in cases showing benign adaptive change.
Also check - SCC Histology: Main Features and Diagnosis
Get Started at ₹1!
Try Flabs for a full month for just ₹1.
Follow us on