Flabs
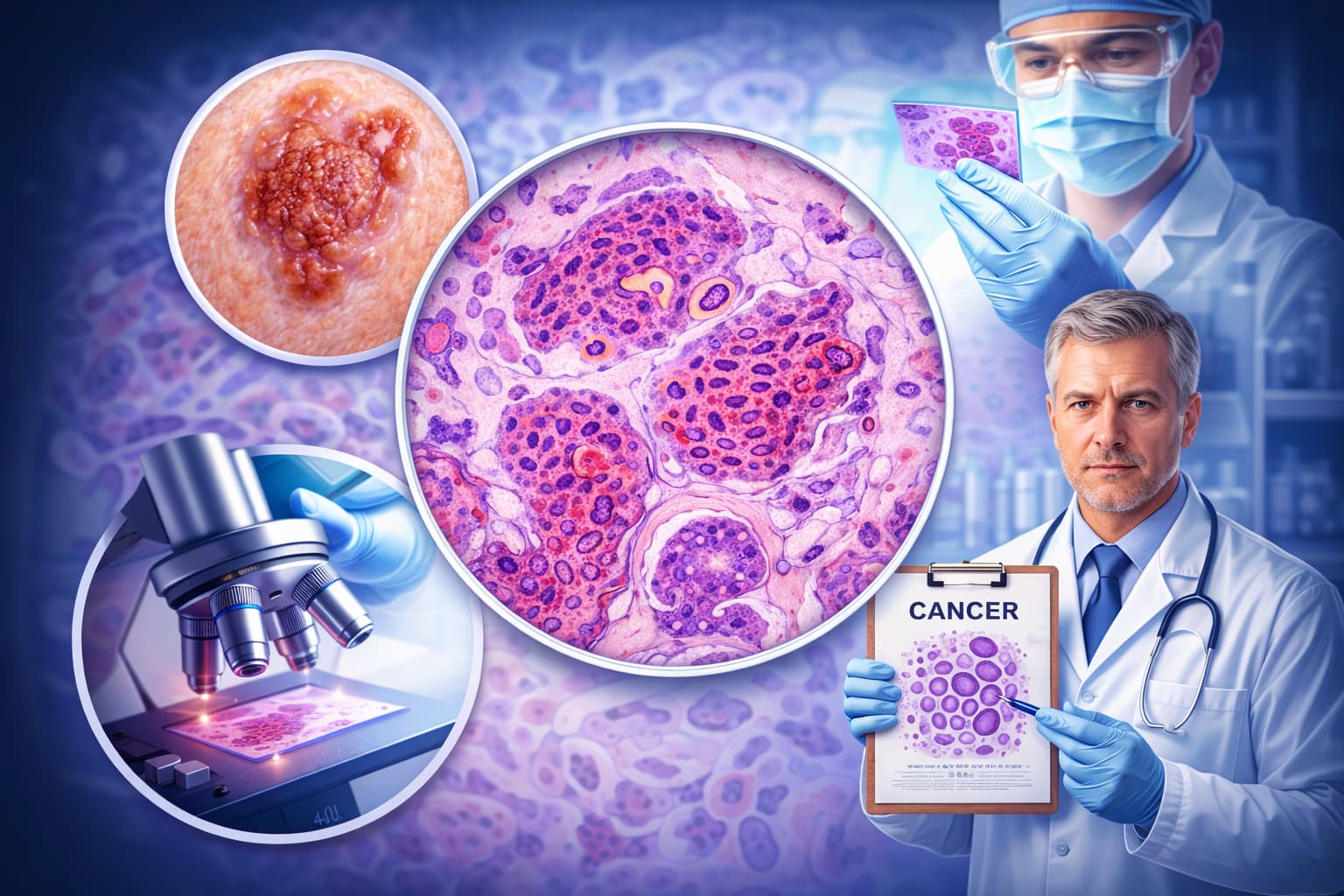
SCC Histology: Main Features and Diagnosis
SCC (Squamous Cell Carcinoma) is generally a type of skin cancer, though it can also form in other areas of the body with mucous membranes. It is the third most common type of cancer in Indian males, with those above 60 years at higher risk.
Indeed, males are at a higher risk of the condition than females. It occurs among people with long-term sun exposure or sun-damaged skin at a young age.
Fortunately, squamous cell carcinoma has an above 80% survival rate with early intervention, where proper diagnosis and treatment play a huge role. The histological spectrum can be surprisingly wide, which poses significant challenges for pathologists and healthcare professionals.
What Is Squamous Cell Carcinoma?
Squamous cell carcinoma (SCC) is a malignant neoplasm arising from squamous epithelial cells. It can develop in any anatomical site lined by squamous epithelium or where squamous metaplasia has occurred, e.g., skin, oral cavity, larynx, oesophagus, cervix, anal cavity, lung, and beyond.
At its histological core, the squamous cell carcinoma meaning refers to a tumour that demonstrates evidence of squamous differentiation: keratin production, intercellular bridges (desmosomes), and the classic architectural patterns you will examine below.
Squamous cell carcinoma causes span a range of molecular and environmental triggers.
- Tobacco and alcohol exposure drive oral and upper aerodigestive tract tumours.
- Human papillomavirus (HPV) drives oropharyngeal and cervical SCCs.
- UV radiation is the main driver of skin SCCs.
Chronic irritation, immunosuppression, and exposure to industrial carcinogens round out the list.
Squamous Cell Carcinoma Histology: Core Features
On H&E sections, squamous cell carcinoma histology presents with a recognisable set of features. The degree to which these features appear depends on the tumour grade.
Histological Features by Grade
| Grade | Histological Features | Clinical Significance |
|---|---|---|
| Well-differentiated (Grade 1) | Abundant keratin pearls, prominent intercellular bridges, low mitotic index, minimal nuclear pleomorphism | Better prognosis; more amenable to surgical resection |
| Moderately differentiated (Grade 2) | Fewer keratin pearls, moderate nuclear pleomorphism, scattered mitoses, recognisable squamous features | Intermediate prognosis; treatment depends on site and stage |
| Poorly differentiated (Grade 3) | Absent or rare keratin pearls, high mitotic rate, marked pleomorphism, sheets of anaplastic cells | Poorer prognosis; may require IHC to confirm squamous lineage |
Site-Specific Histological Patterns
Oral Squamous Cell Carcinoma: Oral squamous cell carcinoma arises most commonly on the lateral tongue, floor of mouth, and lower lip. Histologically, you see irregular invasive nests and cords of malignant squamous cells, desmoplastic stromal reaction, perineural invasion in advanced lesions, and a prominent inflammatory infiltrate at the tumour-stroma interface.
Dysplasia grading in the adjacent mucosa can inform your assessment of the lesion's origin. Squamous cell carcinoma tongue lesions specifically tend to show deeper invasion along muscle planes with correspondingly higher T-stage at diagnosis.
Squamous Cell Lung Carcinoma: Squamous cell lung carcinoma arises centrally from the bronchial epithelium in most cases, although peripheral variants exist. Under the microscope, you will see keratinisation, intercellular bridges, and in advanced cases, cavitation.
You frequently encounter p40 and p63 positivity on IHC. Both are highly specific squamous markers. CK5/6 positivity further confirms lineage.
Distinguishing squamous cell lung carcinoma from adenocarcinoma on biopsy material is essential. It directly determines eligibility for treatment, particularly for EGFR inhibitors and immunotherapy.
Squamous Cell Carcinoma Cytology: What the Smear Tells You
Squamous cell carcinoma cytology on fine needle aspiration or exfoliative samples shows dense orangeophilic cytoplasm (on Pap stain), irregular hyperchromatic nuclei, intercellular bridges when cell groupings are present, and tumour diathesis in the background— necrotic debris and old blood that indicate invasive malignancy.
You may also see tadpole cells and fibre cells— elongated anucleate squamous cells that are characteristic of well-differentiated lesions. In poorly differentiated squamous cell carcinoma cytology, the squamous origin can be less obvious; in these cases, correlate with cell block IHC using p40, CK5/6, and p63 before committing to a final diagnosis.
Symptoms and the Diagnostic Trigger
While symptomatology sits outside pathology's core domain, it shapes your pre-test probability before the specimen reaches you.
Squamous cell carcinoma symptoms vary by site: a non-healing ulcer in the oral cavity, hoarseness from a laryngeal lesion, hemoptysis from a central lung tumour, or a firm nodule with central ulceration on sun-damaged skin.
You can use these inputs to contextualise your histological findings. A well-differentiated keratinising lesion from the oral cavity in a long-term smoker fits a different diagnostic narrative than the same morphology in a non-smoker. And it may prompt reflex HPV testing.
SCC Treatment: How Your Diagnosis Drives Decisions
Your histopathology report directly shapes squamous cell carcinoma treatment. It depends on multiple factors.
- The tumour grade
- Depth of invasion
- Margin status, and
- Presence of lymphovascular and perineural invasion.
Surgery is the primary modality for resectable disease. Radiation therapy is used for locally advanced cases, alone or in combination with platinum-based chemotherapy. Immune checkpoint inhibitors (anti-PD-1/PD-L1 agents) have entered standard care for recurrent or metastatic squamous cell carcinoma at multiple sites. For HPV-positive oropharyngeal lesions, de-escalation protocols are actively being refined based on pathology data.
Accurate grading and margin reporting in your squamous cell carcinoma diagnosis are not formalities. They determine whether your patient gets re-excision, adjuvant radiation, or systemic therapy.
Immunohistochemistry Panel for Confirming SCC
When morphology alone is ambiguous, IHC clarifies the diagnosis. It can happen in poorly differentiated tumours or small biopsies. Your go-to panel for squamous cell carcinoma includes:
P40: Highly specific for squamous differentiation; preferred over p63 in lung.
P63: Sensitive squamous marker; expressed in myoepithelial and urothelial cells as well.
CK5/6: Positive in squamous, basal, and myoepithelial lineages.
CK7 / TTF-1: Usually negative in SCC; positivity should redirect your differential.
HPV ISH or p16 IHC: Reflex testing in oropharyngeal SCC for prognostic stratification.
Pitfalls to Avoid
Pseudoepitheliomatous hyperplasia: It can mimic well-differentiated SCC; look for cytological atypia, atypical mitoses, and stromal desmoplasia to distinguish.
Necrotising sialometaplasia: In salivary tissue, this benign reactive process can look alarming; lobular architecture preservation is your key.
Basaloid SCC: The basaloid variant has a solid growth pattern, comedonecrosis, and focal squamous differentiation; do not confuse with basal cell carcinoma or neuroendocrine carcinoma.
Spindle cell (sarcomatoid) SCC. It requires IHC to confirm; CK AE1/AE3 and p40 are your anchors here.
Faster Histopathology Reporting Starts with Flabs LIS
Every squamous cell carcinoma case you report demands precision and speed. Flabs AI-Powered LIS is built specifically for pathology labs— NABL-trusted and designed to reduce TAT (Turnaround Time) without compromising accuracy.
AI Voice Reporting: Dictate your histological findings naturally. Flabs AI instantly converts your voice into structured, polished diagnostic reports. There’s no typing required during busy sign-out sessions.
AI Interpretation & AI Smart Report: Get AI-generated interpretations aligned to your lab's standards, with fully customisable report templates.
AI Flagger & AI Test Suggestion: Flabs flags abnormal findings and suggests follow-up tests. You never miss a reflex IHC panel or ancillary study on an ambiguous SCC biopsy.
TAT & Quality Control: Track every specimen in real time. Automated QC checks ensure every report meets regulatory standards before delivery.
Dynamic QR Codes & Bulk Sharing: Deliver tamper-proof, QR-coded reports instantly over WhatsApp, SMS, or email, in bulk, with one click.
Start your 5-day free trial today and experience how Flabs transforms your pathology reporting.
Final Word
SCC (Squamous cell carcinoma) is a morphologically diverse malignancy. Your diagnostic accuracy at every stage directly impacts the care your patients receive. Keep grading rigorous, document invasion parameters completely, and correlate with clinical context when the histology is ambiguous. The decisions that follow your report depend on it.
Also check - Cryostat for Histology: Key Benefits & Considerations
Get Started at ₹1!
Try Flabs for a full month for just ₹1.
Follow us on