Flabs
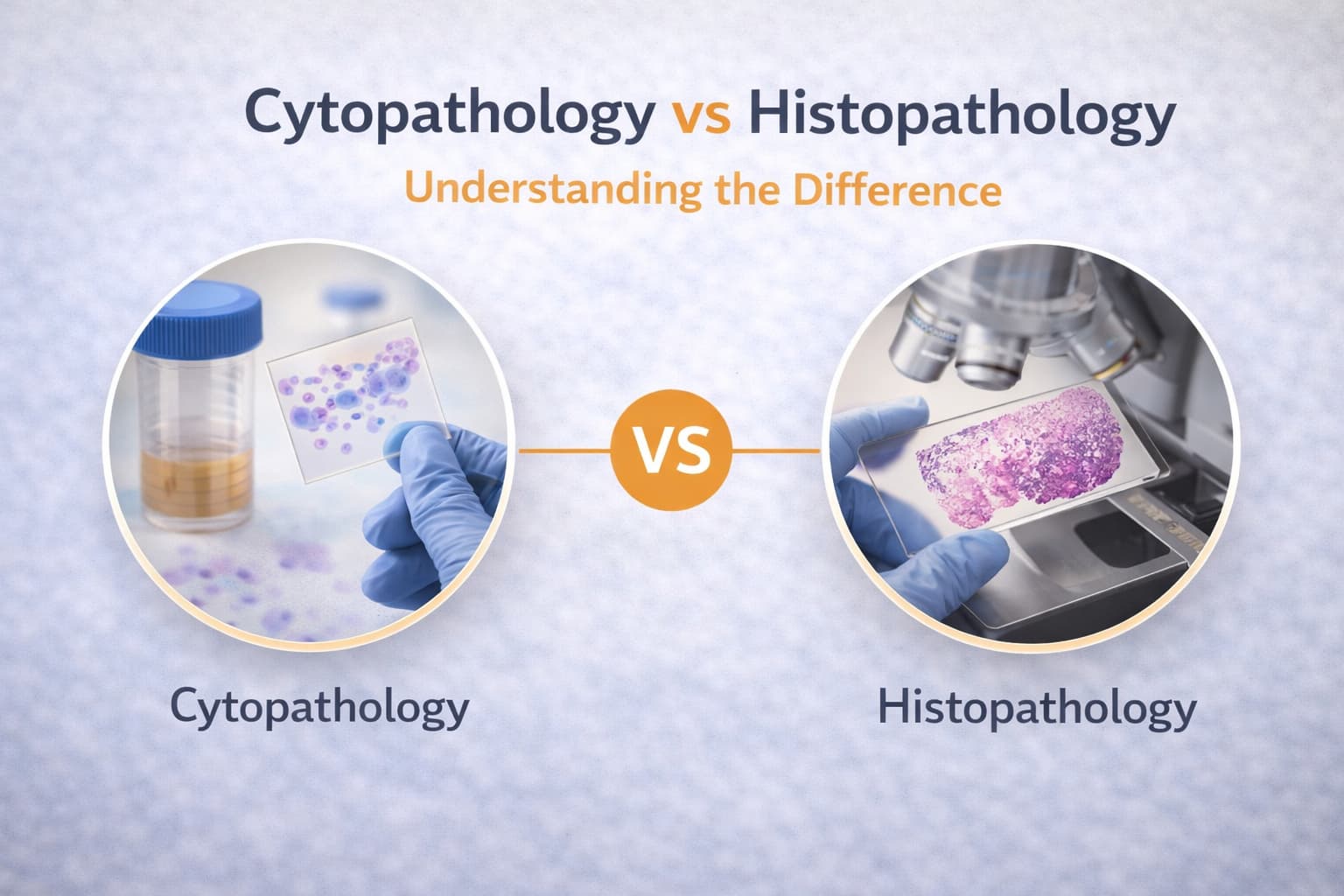
Cytopathology vs Histopathology: Understanding the Difference
As demands grow in diagnostic labs, the role of pathologists and healthcare professionals in selecting the right testing methodology influences both speed and accuracy of patient care. In that line, the decisions around Cytopathology vs histopathology surface every day.
Each method brings its own strengths, limitations, and downstream implications. You may be weighing sample adequacy, procedural risk, turnaround times, or the need for deeper morphologic detail. That’s where a clearer comparison shapes better choices.
A diagnostic strategy gains precision when you match the technique to the clinical question, the sample type, and the therapeutic results. Now, let’s examine how both methods operate, where they diverge, and how modern tools elevate their contribution.
Cytopathology vs Histopathology: At a Glance
| Parameter | Cytopathology | Histopathology |
|---|---|---|
| Sample type | Individual cells, small clusters | Whole tissue sections |
| Procedure invasiveness | Minimal | More invasive |
| Turnaround time | Hours to short days | Longer, except frozen sections |
| Diagnostic accuracy | Moderate (70–80%) | High, with precise classification |
| Structural detail | Limited | Extensive tissue architecture |
| Best suited for | Screening, preliminary evaluation | Confirmation, grading, surgical decisions |
| Ancillary tools | IHC and molecular tests (liquid-based cytology) | IHC, molecular testing, frozen section |
Why the Distinction Matters
You already deal with a demanding diagnostic ecosystem, e.g., compressed timelines, variable sample qualities, and an expanding library of molecular targets.
In that environment, the discussion around cytopathology vs histopathology is not an abstract comparison. It is a practical decision point that influences staging, methods of treatment, and efficiency.
Cytology brings speed and minimal invasiveness, giving you an initial signal.
Histology, on the other hand, delivers architectural detail that anchors classification.
When you weigh the difference between cytopathology and histopathology, the question is how each contributes to the overall diagnostics.
Cytopathology: Cell-Level Detail With Speed
Cytology examines single cells or small cell clusters harvested through FNAC, brushing, scraping, or fluid sampling. The workflow is straightforward and designed for rapid assessment. You may receive interpretable slides within hours to a couple of days.
Main Advantages
- Minimal discomfort for patients.
- Faster sample preparation.
- Lower cost.
- High utility for screening and early detection.
Yet, the limits stand out. Without the benefit of tissue architecture, you work with a narrower context. Diagnostic accuracy is around the 70–80%, influenced by sampling and subjective interpretation. Subtyping cancer becomes more challenging in poorly differentiated lesions.
When liquid-based cytology is used, ancillary assays bring additional resolution. These assays detect protein markers, genetic signals, or actionable mutations, which allows you to refine the preliminary impression provided by morphology alone.
Histopathology: Tissue Architecture and Diagnostic Depth
Histology moves beyond individual cells. You assess full tissue sections, processed through fixation, paraffin embedding, [microtomy](Histopathology: Tissue Architecture and Diagnostic Depth
The payoff is a more definitive diagnosis with strong reproducibility. Cancer classification, grading, and therapeutic stratification depend on these findings. On the other hand, histology demands more from your operational setup, e.g., dedicated lab equipment, personnel, and longer turnaround times.
Frozen sections introduce an exception. Intra-operative evaluation compresses the timeline dramatically. Using a cryostat, tissue is rapidly frozen, cut, stained, and examined. Within 15–20 minutes, you can give the surgical team provisional results for further assessment.
Where Both Techniques Intersect
Although they differ, histopathology and cytopathology operate in a shared lab ecosystem. You may start with cytology for rapid triage and escalate to histology when a full picture is required. Both fields now incorporate analytical and quantitative cytopathology and histopathology methods: digital image analysis, algorithm-based scoring, and semi-automated measurements that support reproducible interpretations.
AI-enabled software platforms extend the workflow further by detecting subtle morphologic cues, assisting with quality assurance, and reporting. These tools don’t replace your expertise; rather, they reduce variability and accelerate interpretation.
Techniques in Histopathology and Cytopathology
Liquid-Based Cytology (LBC): Improves sample preservation and consistency, enabling reflex molecular testing.
Cell Block Preparation: Converts cytology samples into a paraffin-embedded format, creating a hybrid platform for expanded IHC panels.
Special Stains and IHC: Detects protein expression patterns for tumor classification or infectious agent identification.
Molecular Assays: Identifies oncogenic drivers, gene fusions, and microsatellite status.
Digital Pathology: Allows slide scanning, remote review, and quantitative algorithms for cell clustering, nuclear atypia assessment, and more.
When you compare cytopathology vs histopathology within these, the most meaningful divergence lies in how much structural integrity is available for interpretation and which ancillary tools can be applied without compromising the sample.
Role of Ancillary Tests
Modern diagnostics rarely rely on a single stain or morphology alone. You integrate IHC, FISH, PCR-based testing, and next-generation sequencing depending on disease.
In cytology, LBC preparations increase compatibility with these assays. You can obtain biomarkers earlier in the patient journey, reducing delays in treatment planning. Some laboratories now create standardized pathways where abnormal cytology automatically triggers a panel of targeted assays.
In histology, the tissue volume gives greater latitude. Multiple markers, serial sections, and deeper molecular analyses maintain accuracy for tumor typing and prognostication. Tissue architecture also contextualizes molecular findings, reducing false-positive interpretations driven by sampling bias.
Cytopathology’s Role in Early Detection
When screening is the priority cytology is the first line, e.g., cervical cancer or thyroid nodules. The approach balances speed and accessibility. Abnormal findings serve as a prompt for escalation to histology, imaging, or additional sampling.
As research expands, cytology slides are now being incorporated into large datasets for quantitative morphology and algorithm development. These datasets refine automated triaging systems that lighten workload significantly.
Histopathology’s Role in Definitive Classification
Once abnormality is confirmed, you turn to histology for classification and staging. Tissue architecture defines invasion depth, margin status, growth pattern, and stromal reaction.
Frozen sections extend the capability into the operating room. Surgeons value real-time feedback, and you provide it through rapid processing. Although frozen morphology may not match paraffin-embedded quality, it supplies guidance during time-sensitive decisions.
How Technology Elevates the Partnership Between Both Methods
Modern diagnostic software brings cytology and histology into a more integrated workflow. Pattern recognition algorithms reduce variability, while digital reporting systems consolidate images, annotations, and molecular data into a single record.
As laboratories adopt AI-assisted triage, your workload shifts to higher-complexity interpretation. The relationship between cytopathology vs histopathology becomes more complementary than competitive.
Conclusion
When you evaluate cytopathology vs histopathology, the comparison is more of an alignment exercise.
Cytology accelerates early detection; histology confirms and classifies disease; ancillary assays refine the outcome; frozen sections support immediate surgical decisions.
You have to rely on both techniques to deliver clarity at different stages of patient management. As digital tools and quantitative approaches mature, histopathology and cytopathology move toward a more interconnected model across your workflows.
Also read - Decalcification in Histopathology: Why It Matters
Get Started at ₹1!
Try Flabs for a full month for just ₹1.
Follow us on